| Image |
 |
 |
| How the Operation is Done |
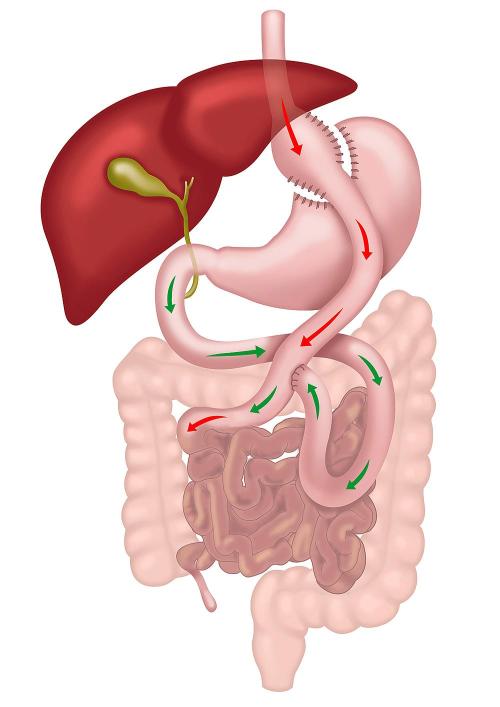
Performed laparoscopically, RYGB involves creating a small stomach pouch and connecting it to the small intestine, bypassing most of the stomach and duodenum with two joints. |
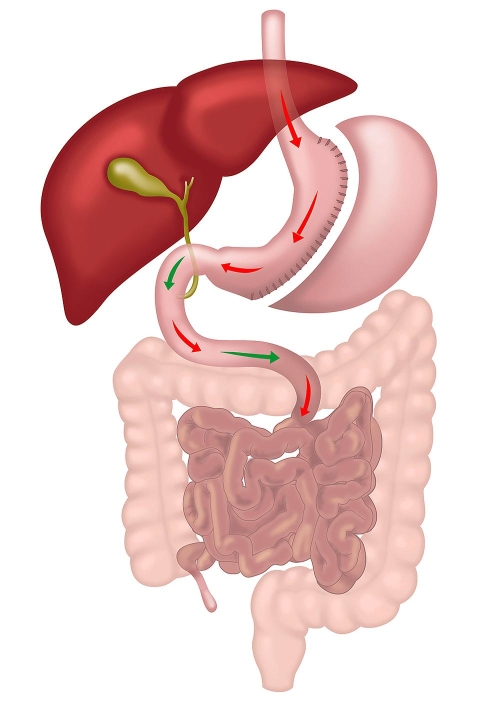
Performed laparoscopically, Sleeve Gastrectomy involves removing a large portion of the stomach, leaving a narrow, tube-like stomach that limits food intake. The small intestine is not altered. |
| Modality of Action |
Restrictive and Metabolic. The metabolic component is stronger than in sleeve due to change in small intestine anatomy. |
Restrictive and Metabolic. The metabolic component is weaker than in gastric bypass as the small intestine is not altered. |
| Weight Loss Potential |
Higher weight loss potential, achieving approximately 30-40% of total body weight due to dual mechanisms of caloric restriction and metabolic changes. |
Moderate weight loss, approximately 25-35% of total body weight, primarily through restriction of food intake. |
| Improvement in Metabolic Conditions |
Greater improvement in conditions like type 2 diabetes, hypertension, and hyperlipidemia due to significant hormonal changes affecting insulin sensitivity and glucose homeostasis. |
Significant improvement in metabolic conditions, but generally less pronounced than with RYGB, as metabolic effects are secondary to the restrictive nature of the procedure. |
| Management of Gastro-Oesophageal Reflux Disease (GORD) |
Effective for GORD management as it reduces acid production and reroutes bile away from the stomach pouch, lowering the risk of acid reflux. |
May worsen or give rise to GORD symptoms due to the high-pressure system created in the sleeved stomach, making it less suitable for patients with existing GORD. |
| Risk of Nutritional Deficiencies |
Higher risk of deficiencies due to bypassed sections of the small intestine, requiring lifelong supplementation and monitoring for vitamins and minerals. |
Lower risk of deficiencies, though supplementation is recommended. Nutrient absorption is less impacted as the small intestine is not bypassed. |
| Complexity of Procedure |
More complex, involving two anastomoses and significant rerouting of the gastrointestinal tract, leading to a higher risk of complications and a longer learning curve for surgeons. |
Less complex, primarily involves reducing the stomach size without altering the intestinal tract, which generally leads to fewer complications. |
| Risk of Marginal Ulcer and Bowel Twist |
Small risk of marginal ulcers at the anastomosis sites and potential for bowel twists or internal hernias due to altered anatomy. |
No risk of marginal ulceration and bowel twist, as the procedure does not alter the small bowel. |
| Can Take Anti-inflammatory Medications? |
No, lifelong restriction due to risk of marginal ulcer. |
Yes |
| Dumping Syndrome |
Common due to rapid gastric emptying into the intestine, leading to symptoms such as nausea, vomiting, diarrhea, and dizziness. |
Rare, as the stomach maintains a more natural function without rapid emptying into the intestine. |
| Limitations on Endoscopic Procedures |
ERCP and other endoscopic procedures are challenging due to altered anatomy, which complicates access to the biliary and pancreatic ducts. |
Normal endoscopic access is maintained, allowing easier management of biliary and pancreatic conditions. |
| Reversibility |
Reversible, but the reversal process is complex and involves significant surgery. |
Non-reversible; however, it can be converted to other operations like RYGB or SADI if needed. |
| Hospital Stay |
2-3 nights on average due to the complexity of the procedure and need for monitoring. |
1-2 nights on average, as the procedure is less invasive with fewer potential complications. |
| Good For |
Patients with severe obesity, type 2 diabetes, and those with GORD or at risk of developing it. |
Patients with moderate obesity without severe GORD, especially those seeking a less complex surgical option. Also as a first step in very big patients. |