| Image |
 |
 |
 |
| How is it done? |
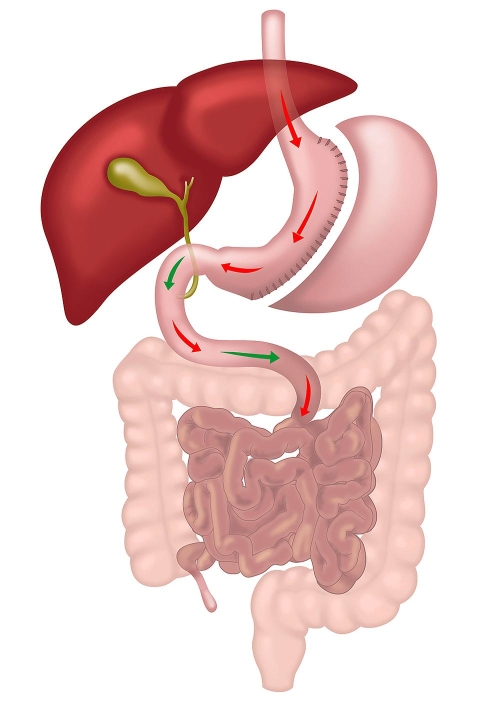
Keyhole surgery |
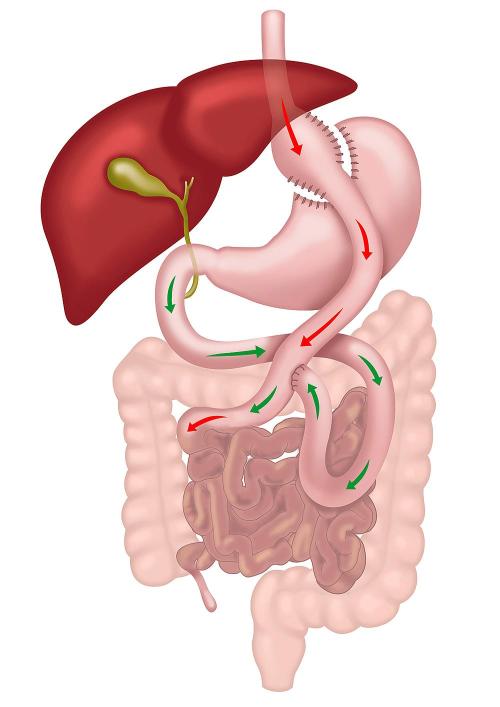
Keyhole surgery with two anastomoses |
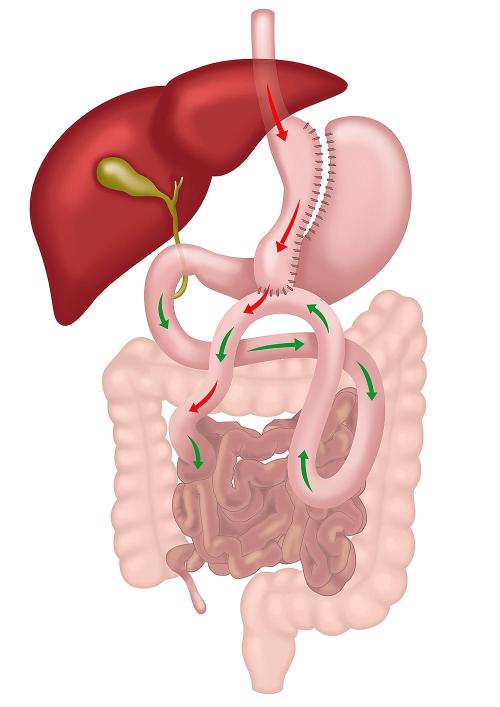
Keyhole surgery with a single anastomosis |
| Modality of Weight Loss |
Restrictive and Metabolic |
Restrictive and Metabolic |
Restrictive and Metabolic |
| How does it work? |
Reduces the stomach to a narrow tube, limiting food intake and reducing ghrelin levels (hunger hormone). |
Creates a small stomach pouch and reroutes the small intestine with two joints. Bile does not reach the stomach pouch. Reduces food intake and induces significant hormonal changes, aiding in appetite suppression and glucose homeostasis. |
Creates a long stomach pouch and joins the small intestine to the stomach pouch. One joint simplifies the operation but brings bile into the stomach pouch. |
| Weight Loss Potential |
Moderate weight loss, around 25-35% of total body weight. |
Higher weight loss potential, around 30-40% of total body weight due to dual mechanisms. |
Similar or even superior weight loss outcomes to RYGB, around 30-40% of total body weight. |
| Improvement in Metabolic Conditions |
Significant improvement in type 2 diabetes, hypertension, and hyperlipidemia. |
More effective improvement in metabolic conditions compared to Sleeve Gastrectomy due to greater changes in gut hormones. |
Comparable or greater improvement in metabolic conditions compared to RYGB, with pronounced hormonal changes. |
| Management of Gastro-Oesophageal Reflux Disease (GORD) |
May worsen or give rise to GORD due to high-pressure system in the sleeved stomach. |
Effective for GORD, as it reduces acid production and diverts bile away from the stomach. |
Risk of bile reflux, which may exacerbate GORD symptoms. |
| Nutritional Deficiencies |
Low to moderate risk of deficiencies; requires some supplementation. |
Higher risk of deficiencies due to bypassed small intestine. Requires lifelong supplementation and monitoring. |
Higher risk of nutritional deficiencies than RYGB due to a longer bypass, requiring regular monitoring and supplementation. |
| Complexity of the Procedure |
Less complex, involving a single reduction of stomach size. |
More complex, involving two anastomoses and rerouting of the gastrointestinal tract. |
Simpler than RYGB, with only one anastomosis, but more complex than Sleeve Gastrectomy. |
| Requires Re-routing of Intestine |
No |
Yes |
Yes |
| Number of Mesenteric Spaces and Risk of Internal Hernias |
None; low risk of internal hernias. |
Two spaces created, increasing the risk of internal hernias. |
One space created, lower risk of internal hernias compared to RYGB. |
| Risk of Malnutrition |
Very low |
Low |
Low but higher than RYGB |
| Risk of Gallstones |
20% |
20% |
20% |
| Main Weakness |
Risk of new onset or worsening of GORD (acid reflux) in 25% of patients. |
More complex surgery with a higher risk of internal hernias and nutritional deficiencies. |
Risk of bile reflux and a slightly higher risk of malnutrition compared to RYGB. |
| Can Take Anti-inflammatory Medications |
Yes |
No, lifelong restriction due to risk of marginal ulcer. |
No, lifelong restriction due to risk of marginal ulcer. |
| Risk of Marginal Ulceration |
Rare |
Moderate; smaller stomach pouch helps reduce acid production. |
Higher risk due to larger pouch and bile exposure. |
| Dumping Syndrome |
Rare |
Common due to rapid gastric emptying into the intestine. |
Less common than RYGB, but still possible due to the bypass. |
| Need for Multivitamins Lifelong |
Possibly no |
Yes |
Yes |
| Reversibility |
No, but convertible to other operations such as RYGB, OAGB, or SADI. |
Yes, but difficult. |
Yes, less difficult than RYGB. |
| Limitations on Endoscopic Procedures |
Normal endoscopic access is maintained. |
Limited access for ERCP due to altered anatomy, making it challenging. |
Limited access for ERCP, but potentially easier than RYGB due to a simpler anatomy. |
| Operating Time |
1 hour |
2-3 hours |
1-2 hours |
| Advantages |
Reduces hunger, normal sensation of fullness, no food intolerance, no foreign body, improves diabetes, "Set and forget" operation, less follow-up needed. |
Best long-term data, more effective for metabolic conditions, improves diabetes quickly, fixes acid reflux, lower risk of bile reflux. |
Shorter operation time, effective in weight loss and diabetes control, simpler surgery with potential for reversibility, lower risk of internal hernias. |
| Disadvantages & Complications |
Staple line leak, narrowing, rare GORD. |
Staple line leak, ulcers, dumping syndrome, nutritional deficiencies, internal hernias. |
Risk of bile reflux, staple line leak, nutritional deficiencies, close monitoring needed for malabsorption. |
| Long-term Need for Re-operation |
Very rare |
5-10% over ten years |
Less than 5% over ten years |
| Average Hospital Stay |
1-2 nights |
2-3 nights |
2-3 nights |
| Quality of Life |
Best among weight loss operations |
Good, but dumping syndrome can be an issue |
Good; generally less dumping syndrome, but bile reflux can be an issue |
| Average Weight Loss |
25-35% of total body weight |
30-40% of total body weight |
30-40% of total body weight |
| Good for |
Non-diabetics and with no or minimal reflux. |
Diabetics or patients with significant acid reflux. |
Diabetics and without significant reflux. |