| Feature | Roux-en-Y Gastric Bypass (RYGB) | One Anastomosis Gastric Bypass (OAGB) | Notes |
|---|---|---|---|
| Image |
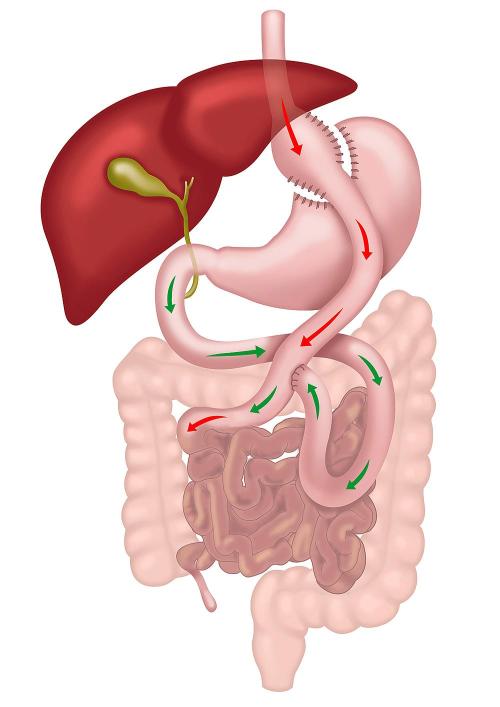
Roux-en-Y Gastric Bypass (RYGB) |
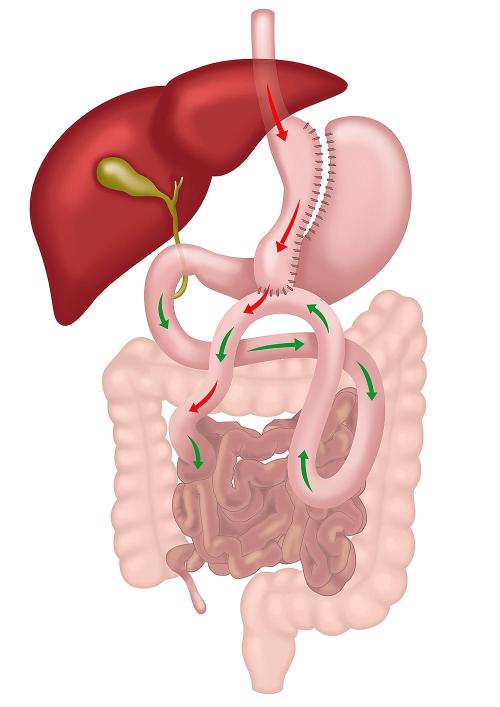
One Anastomosis Gastric Bypass (OAGB) |
|
| Mechanism of Action | Restricts food intake and reroutes small bowel to bypass absorption sites. | Restricts food intake with a single connection bypassing absorption sites. | Both induce hormonal changes (e.g., increased GLP-1, reduced ghrelin), improving satiety and glucose metabolism. |
| Stomach Modification | Small and narrow gastric pouch created (~30 mL). | Long narrow gastric pouch created (~150 mL). | OAGB pouch is longer compared to RYGB. |
| Number of Anastomoses | Two (gastrojejunal and jejunojejunal). | One (gastrointestinal). | The single anastomosis in OAGB simplifies the procedure and reduces operative time. |
| Bile Reflux | Rare. | Possible due to single anastomosis. | Bile reflux is a significant consideration in OAGB and may require revision surgery in symptomatic cases. |
| Risk of Marginal Ulcers | Small. | Small but likely higher than RYGB due to bile and acid exposure at the single anastomosis. | In both operations, the risk of marginal ulcers is higher in smokers or with use of NSAIDs (anti-inflammatory drugs). |
| Weight Loss Outcomes | 70–80% excess weight loss (EWL) or 30–40% of total body weight. | 70–80% excess weight loss (EWL) or 30–40% of total body weight. | Comparable weight loss outcomes in the first 2 years; durability varies depending on individual factors and compliance with lifestyle changes. |
| Improvement in Metabolic Conditions | Significant improvement in type II diabetes, insulin resistance, and metabolic syndrome. | Significant improvement in type II diabetes, insulin resistance, and metabolic syndrome. | Both procedures improve glucose homeostasis through hormonal changes and weight loss, often leading to remission of type II diabetes. |
| Risk of Internal Hernias | Higher due to two mesenteric defects. | Lower due to one mesenteric defect. | RYGB has a higher risk of hernias requiring surgical intervention. |
| Risk of Gastroesophageal Reflux Disease (GERD) | Reduced in most patients. | Bile reflux may mimic or worsen GERD symptoms. | Both can improve GERD, but OAGB's bile reflux risk can be problematic for some patients. |
| Suitability for NSAIDs | Contraindicated. | Contraindicated. | NSAID use is not advised in either procedure due to the increased risk of marginal ulcers. |
| Revisional Surgery Risk | Moderate. | Moderate. | Both procedures can require revisions for complications such as reflux, malnutrition, or inadequate weight loss. |