| Aspect | Roux-en-Y Gastric Bypass (RYGB) | Sleeve Gastrectomy |
|---|---|---|
| Image | 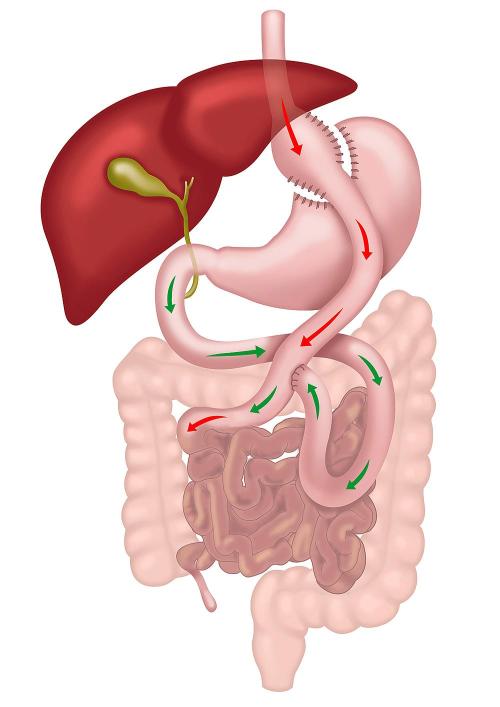 |
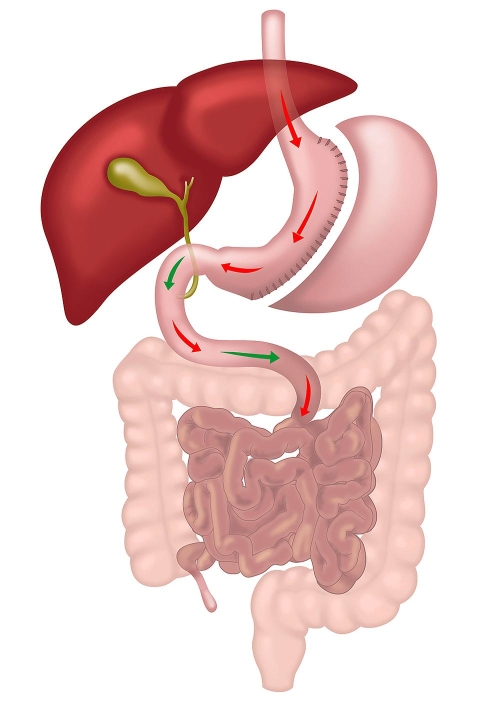 |
| How the Operation is Done | Performed laparoscopically, RYGB involves creating a small stomach pouch and connecting it to the small intestine, bypassing most of the stomach and duodenum with two joints. | Performed laparoscopically, Sleeve Gastrectomy involves removing a large portion of the stomach, leaving a narrow, tube-like stomach that limits food intake. The small intestine is not altered. |
| Modality of Action | Restrictive and Metabolic. The metabolic component is stronger than in sleeve due to change in small intestine anatomy. | Restrictive and Metabolic. The metabolic component is weaker than in gastric bypass as the small intestine is not altered. |
| Weight Loss Potential | Higher weight loss potential, achieving approximately 30-40% of total body weight due to dual mechanisms of caloric restriction and metabolic changes. | Moderate weight loss, approximately 25-35% of total body weight, primarily through restriction of food intake. |
| Improvement in Metabolic Conditions | Greater improvement in conditions like type 2 diabetes, hypertension, and hyperlipidemia due to significant hormonal changes affecting insulin sensitivity and glucose homeostasis. | Significant improvement in metabolic conditions, but generally less pronounced than with RYGB, as metabolic effects are secondary to the restrictive nature of the procedure. |
| Management of Gastro-Oesophageal Reflux Disease (GORD) | Effective for GORD management as it reduces acid production and reroutes bile away from the stomach pouch, lowering the risk of acid reflux. | May worsen or give rise to GORD symptoms due to the high-pressure system created in the sleeved stomach, making it less suitable for patients with existing GORD. |
| Risk of Nutritional Deficiencies | Higher risk of deficiencies due to bypassed sections of the small intestine, requiring lifelong supplementation and monitoring for vitamins and minerals. | Lower risk of deficiencies, though supplementation is recommended. Nutrient absorption is less impacted as the small intestine is not bypassed. |
| Complexity of Procedure | More complex, involving two anastomoses and significant rerouting of the gastrointestinal tract, leading to a higher risk of complications and a longer learning curve for surgeons. | Less complex, primarily involves reducing the stomach size without altering the intestinal tract, which generally leads to fewer complications. |
| Risk of Marginal Ulcer and Bowel Twist | Small risk of marginal ulcers at the anastomosis sites and potential for bowel twists or internal hernias due to altered anatomy. | No risk of marginal ulceration and bowel twist, as the procedure does not alter the small bowel. |
| Can Take Anti-inflammatory Medications? | No, lifelong restriction due to risk of marginal ulcer. | Yes |
| Dumping Syndrome | Common due to rapid gastric emptying into the intestine, leading to symptoms such as nausea, vomiting, diarrhea, and dizziness. | Rare, as the stomach maintains a more natural function without rapid emptying into the intestine. |
| Limitations on Endoscopic Procedures | ERCP and other endoscopic procedures are challenging due to altered anatomy, which complicates access to the biliary and pancreatic ducts. | Normal endoscopic access is maintained, allowing easier management of biliary and pancreatic conditions. |
| Reversibility | Reversible, but the reversal process is complex and involves significant surgery. | Non-reversible; however, it can be converted to other operations like RYGB or SADI if needed. |
| Hospital Stay | 2-3 nights on average due to the complexity of the procedure and need for monitoring. | 1-2 nights on average, as the procedure is less invasive with fewer potential complications. |
| Good For | Patients with severe obesity, type 2 diabetes, and those with GORD or at risk of developing it. | Patients with moderate obesity without severe GORD, especially those seeking a less complex surgical option. Also as a first step in very big patients. |
Hydration
- By now, drinking fluids should feel much easier than in the early weeks after surgery.
- Staying properly hydrated is essential for healing, digestion, and energy levels. Aim to drink at least 1.5 to 2 litres of fluids per day.
- A simple way to check your hydration status is the colour of your urine. It should be pale yellow—if it is dark, you need to drink more water.
Diet: Transitioning to Solid Foods
- Start introducing solid foods into your diet gradually. Begin with fish, then chicken, and then red meat.
- Protein-based foods should be the foundation of your long-term diet. Every meal should prioritise protein sources like lean meats, eggs, dairy, tofu, and legumes.
- Introduce new foods carefully. Start with a small portion of any new food and give your stomach plenty of time to adjust.
- Limit carbohydrates such as potato, bread, pasta, and rice as they can expand in your stomach, making it harder to consume enough protein.
- Use the Portion Perfection Plate and Bowl (provided in your pre-op green bag) to help with food selection and portion sizes.
- Hunger may start to return as your stomach heals. Avoid unnecessary cravings by limiting exposure to food-related TV shows, cooking videos, and advertisements.
Multivitamins and Supplements
- Continue taking your bariatric multivitamins twice a day—this is essential for preventing vitamin and mineral deficiencies.
- Many patients switch from chewable vitamins to capsules at this stage. If you find capsules easier to swallow, you can try BN Multi Capsules (formulated for bariatric patients).
- Some patients may require additional supplements such as Iron, Calcium, Vitamin D, and B12 injections. Your blood tests will help determine if you need these.
Exercise: Building Strength and Stamina
- From six weeks after surgery, there are no restrictions on activities.
- Consistency matters—regular, moderate exercise is more effective than intense but infrequent workouts.
- Aim for at least 20-30 minutes of brisk activity 5 times per week. Walking, swimming, or cycling are excellent options.
- Strength training (using light weights, resistance bands, or bodyweight exercises) helps rebuild muscle and boosts metabolism.
- If you still feel fatigued, focus on hydration, protein intake, and gradual increases in activity.
Pain and Gallstones
- By now, pain should be minimal or completely gone.
- Some patients who had gallstones before surgery may begin experiencing gallbladder attacks (pain in the upper abdomen and back).
- By six months post-op, about 20% of patients will develop gallstones due to rapid weight loss. These stones can cause pain if they block the bile duct.
- If you still have your gallbladder and had no gallstones on your pre-op scan, we will arrange an abdominal ultrasound before your 6-month review to check for new stones.
- If gallstones become painful, gallbladder removal may be necessary.
Acid Reflux (Heartburn)
- Continue taking Nexium (or another PPI) daily until at least 3 months post-op.
- If heartburn persists after 3 months, continue Nexium as needed and discuss with your surgeon if symptoms persist.
- Over time, as your stomach heals and becomes more flexible, reflux should improve.
- To prevent acid reflux: Do not eat or drink for at least one hour before bedtime. Avoid spicy, acidic, or fatty foods.
Vomiting
- Vomiting should not be common at this stage.
- It may happen if eating or drinking too quickly, or eating too much.
- To avoid vomiting: Eat slowly, chew food thoroughly, and stop eating at the first sign of feeling full.
Hair Loss After Surgery
- Temporary hair loss is common during the first year after surgery.
- This is due to the stress of surgery and rapid weight loss, similar to postpartum hair loss.
- Hair will regrow fully within 9-12 months.
- Extra vitamins or protein supplements will not prevent hair loss, but adequate protein intake and multivitamins are essential for overall health.
Tracking Your Weight Loss Progress
- Weigh yourself only once a week using the same scales, at the same time each week.
- Taking monthly progress photos can help you see changes that the scale doesn’t reflect.
- Weight loss is not always linear—some weeks you may not see much change, while other weeks will show bigger drops.
Follow-Up Appointments
- You will have an appointment with your surgeon, nurse, and dietitian around the 6-8 month mark.
- Before your appointment: Complete blood tests at least one week prior.
- If you still have your gallbladder, schedule an upper abdominal ultrasound two weeks before your appointment.

Introduction
Gastric bypass surgery is a major step toward improving health for people with obesity. While it often leads to significant weight loss and better management of conditions like diabetes and high blood pressure, it also changes the way your body absorbs medications. Understanding these changes is crucial for ensuring continued benefits without unexpected side effects. This article explains what happens to medications after gastric bypass, why some medications might need adjustments, and how you and your healthcare team can manage this process effectively.
The information in this article applies to patients who have undergone Roux-en-Y gastric bypass, one anastomosis gastric bypass, or the SADI operation, as these procedures alter the small bowel and significantly affect medication absorption. In contrast, sleeve gastrectomy does not alter the small bowel and generally has little effects on medication absorption.
Section 1: What Is Gastric Bypass Surgery?
Overview of Roux-en-Y Gastric Bypass (RYGB)
Roux-en-Y gastric bypass (RYGB) is one of the most common and effective weight-loss surgeries. It involves creating a small stomach pouch that is connected directly to the middle part of the small intestine, bypassing most of the stomach and the upper small intestine (duodenum).
- Smaller Stomach Pouch: The new stomach pouch, about the size of an egg, restricts food intake.
- Bypassing the Small Intestine: This reduces nutrient and medication absorption, aiding weight loss but affecting medication effectiveness.
Key Physiological Changes After Surgery
Gastric bypass causes several changes in the body:
- Reduced Acid Production: Less acid in the smaller stomach pouch affects medication breakdown.
- Faster Gastric Emptying: Medications spend less time in the stomach, impacting absorption.
- Hormonal Changes: Reduced hunger hormones (e.g., ghrelin) also influence drug processing.
- Decreased Bile Flow: Reduced bile impacts the absorption of fatty medications and fat-soluble vitamins (A, D, E, K).
Summary: After RYGB, medications may not be absorbed as they were before, potentially reducing their effectiveness. Patients may need changes in dosage or formulation to maintain proper treatment.
Section 2: How Gastric Bypass Affects Your Medications
Why Medication Adjustments Are Necessary
Gastric bypass changes the digestive process, altering how medications are absorbed:
- Reduced Absorption: Medications needing an acidic environment or absorption in the upper small intestine (e.g., digoxin, ketoconazole) may become less effective.
- Increased Absorption: Some medications, like metformin, may be absorbed faster, leading to stronger effects.
- Unchanged Absorption: Certain medications (e.g., paracetamol) may have similar absorption before and after surgery.
Managing Medication Changes
Close collaboration with your healthcare team is crucial to avoid underdosing or overdosing:
- Adjusting Dosages: Many medications, like insulin or blood pressure medicines, may require dose reduction as weight loss progresses.
- Changing Formulations: Liquid, chewable, or dissolvable medications are often more suitable after surgery.
- Frequent Monitoring: Regular check-ups and blood tests help ensure medications are effective and safe.
Summary: The altered absorption of medications requires careful monitoring, dosage adjustments, and sometimes changes in medication form (e.g., to liquids or chewables).
Section 3: General Principles of Medication Management Post-Gastric Bypass
Key Strategies
- Use Liquid, Chewable, or Dissolvable Medications: These forms are better absorbed in the smaller stomach pouch.
- Avoid Large Tablets: Large pills can cause discomfort or blockages in the smaller stomach pouch.
- Prefer Immediate-Release Formulations: These work better than extended-release forms, which may not be fully absorbed.
- Stay Hydrated: Take medications with adequate water, but avoid drinking large amounts at once to prevent discomfort.
Summary: Switching to smaller, easier-to-absorb medications and regularly monitoring effectiveness is key to safe medication management post-surgery.
Section 4: Practical Medication Management by Drug Class
1. Diabetes Medications
- Insulin: Doses may be lowered by up to 50% after surgery.
- Key Tip: Regular blood glucose monitoring is crucial.
- Oral Antidiabetics: Switch to immediate-release metformin; reduce or stop sulphonylureas.
- GLP-1 Agonists and SGLT2 Inhibitors: May need dose adjustments or discontinuation.
Summary: Rapid weight loss often necessitates significant changes to diabetes medications, especially in the first few months.
2. Blood Pressure Medications
- Antihypertensives: Dose reductions or discontinuation may be needed.
- Diuretics: Use with caution to avoid dehydration.
- ACE Inhibitors/ARBs: May still be beneficial for kidney protection.
Summary: As blood pressure decreases with weight loss, expect medication adjustments and regular monitoring.
3. Pain Relief (Analgesics)
- Paracetamol: Safe and effective.
- NSAIDs: You should not take NSAIDs for life after gastric bypass due to a high risk of stomach irritation, ulcers, and bleeding.
- Alternative Options: Short-term use of opioid analgesics may be needed but must be monitored closely.
- Low-Dose Aspirin: Low-dose aspirin (100 to 150 mg per day) used to thin the blood in patients with ischemic heart disease, peripheral vascular disease, or cerebrovascular disease is safe and can be continued.
Summary: Paracetamol is the preferred option for pain relief; avoid NSAIDs permanently to prevent serious complications but low-dose aspirin can be continued for specific conditions.
4. Antidepressants and Anxiety Medications
- SSRIs/SNRIs: May need dose increases due to reduced absorption.
- Tricyclics: Careful monitoring is needed to manage side effects.
- Benzodiazepines: Prefer liquid forms; monitor for dependency.
Summary: Careful monitoring is needed for effective management of mental health medications post-surgery.
5. Anticonvulsants (Anti-Epileptic Medications)
- Reduced Absorption: After gastric bypass, the absorption of anticonvulsants is reduced, which can make them less effective.
- Advice: Patients should see their GP regularly to have their blood levels checked and adjust doses as needed.
- Monitoring: Close monitoring of seizure control is essential.
Summary: Regular blood level checks are necessary to maintain effective seizure control after surgery.
6. Lithium
- Narrow Therapeutic Range: Lithium requires careful management, as changes in absorption can lead to toxicity or ineffective treatment.
- Advice: Regular blood tests to monitor lithium levels are crucial, with potential dose adjustments to maintain stability.
Summary: Frequent monitoring and dose adjustments are essential for safe lithium use post-surgery.
7. Proton Pump Inhibitors (PPIs) (e.g., Nexium, Pariet, Omeprazole)
- Reduced Absorption: PPIs are enteric-coated and may not be fully absorbed after gastric bypass.
- Advice: Patients should crush, chew, or dissolve these medications before swallowing to ensure effective absorption.
Summary: Alter the form of PPIs to improve absorption and maintain their effectiveness post-surgery.
8. Anticoagulants and Antiplatelets
- Warfarin: Often preferred due to ease of monitoring (INR).
- DOACs: Absorption may be altered, requiring dose adjustments.
Summary: Close monitoring of blood clotting parameters is essential to maintain safety with blood thinners.
Section 5: Special Considerations After Gastric Bypass Surgery
1. Vitamin and Mineral Supplementation
- Essential Supplements:
- Calcium citrate, Vitamin D, Vitamin B12, Iron, and multivitamins.
- Take Vitamin B12 sublingually or via injections for better absorption.
- Separate calcium and iron by at least 2 hours.
Summary: Regular blood tests and consistent supplement intake are necessary to prevent deficiencies.
2. Alcohol and Substance Use
- Alcohol Absorption: Increases after surgery, leading to faster intoxication.
- Avoid Addiction Transfer: Be aware of potential shifts from food to alcohol dependence.
Summary: Limit alcohol intake, monitor its effects, and seek support if needed.
Section 6: Top 10 Medication Tips After Gastric Bypass
- Use liquid, chewable, or dissolvable medications whenever possible.
- Avoid extended-release formulations; opt for immediate-release instead.
- Space out medications throughout the day to prevent overfilling the stomach pouch.
- Separate calcium supplements from other medications by 2 hours.
- Do not take NSAIDs for life due to ulcer risks. Continue low dose aspirin for ischemic heart disease or vascular disease.
- Monitor blood glucose regularly if you have diabetes.
- Have regular blood tests for anticonvulsants and lithium to ensure correct dosing.
- Crush, chew, or dissolve PPIs before taking them for better absorption.
- Attend regular follow-ups with your healthcare team.
- Communicate any changes in symptoms or medication effects promptly.
Section 7: Clinical Monitoring and Follow-Up
Regular Monitoring
- First 6-12 Months: Frequent follow-ups every few weeks to monitor progress and adjust medications.
- Long-Term: Regular weight, blood pressure, and blood test monitoring.
Summary: Ongoing monitoring and coordinated care with healthcare providers are essential for successful medication management post-surgery.
Comparison of Bariatric Procedures
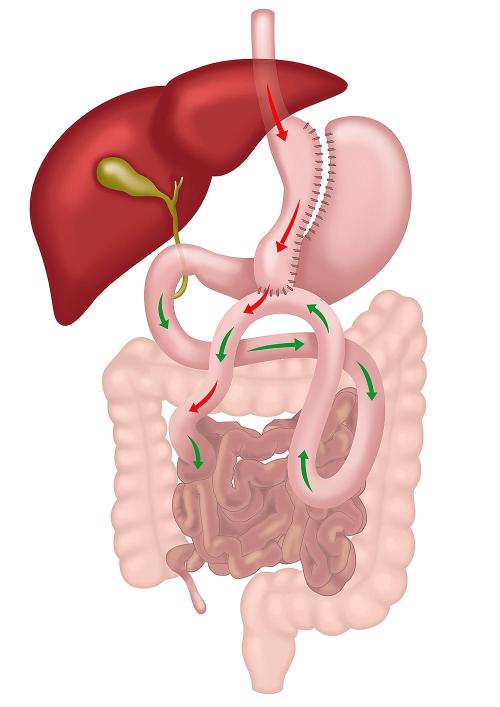
| Name of Operation | Sleeve Gastrectomy | Roux-en-Y Gastric Bypass (RYGB) | One Anastomosis Gastric Bypass (OAGB) |
|---|---|---|---|
| Image | |
|
 |
| How is it done? | Keyhole surgery | Keyhole surgery with two anastomoses | Keyhole surgery with a single anastomosis |
| Modality of Weight Loss | Restrictive and Metabolic | Restrictive and Metabolic | Restrictive and Metabolic |
| How does it work? | Reduces the stomach to a narrow tube, limiting food intake and reducing ghrelin levels (hunger hormone). | Creates a small stomach pouch and reroutes the small intestine with two joints. Bile does not reach the stomach pouch. Reduces food intake and induces significant hormonal changes, aiding in appetite suppression and glucose homeostasis. | Creates a long stomach pouch and joins the small intestine to the stomach pouch. One joint simplifies the operation but brings bile into the stomach pouch. |
| Weight Loss Potential | Moderate weight loss, around 25-35% of total body weight. | Higher weight loss potential, around 30-40% of total body weight due to dual mechanisms. | Similar or even superior weight loss outcomes to RYGB, around 30-40% of total body weight. |
| Improvement in Metabolic Conditions | Significant improvement in type 2 diabetes, hypertension, and hyperlipidemia. | More effective improvement in metabolic conditions compared to Sleeve Gastrectomy due to greater changes in gut hormones. | Comparable or greater improvement in metabolic conditions compared to RYGB, with pronounced hormonal changes. |
| Management of Gastro-Oesophageal Reflux Disease (GORD) | May worsen or give rise to GORD due to high-pressure system in the sleeved stomach. | Effective for GORD, as it reduces acid production and diverts bile away from the stomach. | Risk of bile reflux, which may exacerbate GORD symptoms. |
| Nutritional Deficiencies | Low to moderate risk of deficiencies; requires some supplementation. | Higher risk of deficiencies due to bypassed small intestine. Requires lifelong supplementation and monitoring. | Higher risk of nutritional deficiencies than RYGB due to a longer bypass, requiring regular monitoring and supplementation. |
| Complexity of the Procedure | Less complex, involving a single reduction of stomach size. | More complex, involving two anastomoses and rerouting of the gastrointestinal tract. | Simpler than RYGB, with only one anastomosis, but more complex than Sleeve Gastrectomy. |
| Requires Re-routing of Intestine | No | Yes | Yes |
| Number of Mesenteric Spaces and Risk of Internal Hernias | None; low risk of internal hernias. | Two spaces created, increasing the risk of internal hernias. | One space created, lower risk of internal hernias compared to RYGB. |
| Risk of Malnutrition | Very low | Low | Low but higher than RYGB |
| Risk of Gallstones | 20% | 20% | 20% |
| Main Weakness | Risk of new onset or worsening of GORD (acid reflux) in 25% of patients. | More complex surgery with a higher risk of internal hernias and nutritional deficiencies. | Risk of bile reflux and a slightly higher risk of malnutrition compared to RYGB. |
| Can Take Anti-inflammatory Medications | Yes | No, lifelong restriction due to risk of marginal ulcer. | No, lifelong restriction due to risk of marginal ulcer. |
| Risk of Marginal Ulceration | Rare | Moderate; smaller stomach pouch helps reduce acid production. | Higher risk due to larger pouch and bile exposure. |
| Dumping Syndrome | Rare | Common due to rapid gastric emptying into the intestine. | Less common than RYGB, but still possible due to the bypass. |
| Need for Multivitamins Lifelong | Possibly no | Yes | Yes |
| Reversibility | No, but convertible to other operations such as RYGB, OAGB, or SADI. | Yes, but difficult. | Yes, less difficult than RYGB. |
| Limitations on Endoscopic Procedures | Normal endoscopic access is maintained. | Limited access for ERCP due to altered anatomy, making it challenging. | Limited access for ERCP, but potentially easier than RYGB due to a simpler anatomy. |
| Operating Time | 1 hour | 2-3 hours | 1-2 hours |
| Advantages | Reduces hunger, normal sensation of fullness, no food intolerance, no foreign body, improves diabetes, "Set and forget" operation, less follow-up needed. | Best long-term data, more effective for metabolic conditions, improves diabetes quickly, fixes acid reflux, lower risk of bile reflux. | Shorter operation time, effective in weight loss and diabetes control, simpler surgery with potential for reversibility, lower risk of internal hernias. |
| Disadvantages & Complications | Staple line leak, narrowing, rare GORD. | Staple line leak, ulcers, dumping syndrome, nutritional deficiencies, internal hernias. | Risk of bile reflux, staple line leak, nutritional deficiencies, close monitoring needed for malabsorption. |
| Long-term Need for Re-operation | Very rare | 5-10% over ten years | Less than 5% over ten years |
| Average Hospital Stay | 1-2 nights | 2-3 nights | 2-3 nights |
| Quality of Life | Best among weight loss operations | Good, but dumping syndrome can be an issue | Good; generally less dumping syndrome, but bile reflux can be an issue |
| Average Weight Loss | 25-35% of total body weight | 30-40% of total body weight | 30-40% of total body weight |
| Good for | Non-diabetics and with no or minimal reflux. | Diabetics or patients with significant acid reflux. | Diabetics and without significant reflux. |
SADI-S and Sleeve Gastrectomy (SG) are both popular bariatric procedures aimed at significant weight loss and improving obesity-related health conditions. While SG is a simpler and less invasive operation, SADI-S offers additional benefits due to its combined approach of restriction and malabsorption. Understanding the differences between these procedures in terms of benefits, side effects, and potential complications can help patients and healthcare providers determine the most appropriate choice.
Benefits of SADI-S Compared to Sleeve Gastrectomy
- Enhanced Weight Loss
SADI-S combines two mechanisms for weight loss: restriction (by reducing stomach size) and malabsorption (by bypassing a portion of the small intestine). This dual approach generally leads to more substantial weight loss compared to SG, which only restricts food intake by reducing the size of the stomach.
SG is effective for weight loss, but for patients requiring more significant weight reduction, especially those with a higher body mass index (BMI), SADI-S may offer better outcomes.
- Improved Metabolic Outcomes
SADI-S not only restricts the amount of food that can be consumed but also changes the hormonal environment of the gut, resulting in greater improvements in metabolic conditions such as type 2 diabetes. The hormonal changes from rerouting the intestines promote increased levels of GLP-1 and PYY, which help control blood sugar and appetite.
SG also reduces levels of ghrelin (a hunger hormone), but the hormonal changes are less pronounced compared to SADI-S, making SADI-S more effective for patients with poorly controlled diabetes or other metabolic conditions.
Side Effects of SADI-S Compared to Sleeve Gastrectomy
- Higher Risk of Malabsorption
While the addition of malabsorption in SADI-S enhances weight loss, it also increases the risk of nutritional deficiencies. Patients undergoing SADI-S are at higher risk of deficiencies in essential nutrients like iron, vitamin B12, calcium, and fat-soluble vitamins (A, D, E, K).
SG does not involve intestinal bypass and therefore has a lower risk of nutritional deficiencies. Patients undergoing SG generally only require basic vitamin and mineral supplementation.
- Diarrhoea and Steatorrhoea
The shorter length of the small intestine available for nutrient absorption in SADI-S can lead to diarrhoea or fatty stools (steatorrhoea), especially with high-fat diets. Adherence to dietary recommendations and regular follow-up is essential to manage these symptoms.
In SG, changes in bowel habits are usually less pronounced, with most patients experiencing manageable symptoms such as mild constipation or occasional diarrhoea.
Complications of SADI-S Compared to Sleeve Gastrectomy
- Duodenal Stump Blowout (SADI-S Specific)
SADI-S carries a unique risk of duodenal stump blowout, which occurs when there is a leak or rupture at the closed end of the divided duodenum. This serious complication can lead to peritonitis and sepsis, requiring urgent surgical intervention. This complication is not encountered in SG since the duodenum is not transected in that procedure.
- Anastomotic Leaks
SADI-S involves creating an anastomosis between the duodenum and the ileum, which carries a risk of leaks at the connection site. Prompt recognition and management of leaks are crucial to prevent severe complications.
SG does not involve an intestinal anastomosis, reducing the risk of leaks compared to SADI-S. However, there is still a risk of staple line leaks where the stomach is cut and stapled.
- Nutritional Deficiencies
SADI-S patients face a higher risk of developing nutritional deficiencies due to the bypass of a significant portion of the small intestine. This requires lifelong supplementation and close follow-up to monitor nutrient levels.
While SG patients also need supplementation, the risk of severe deficiencies is lower compared to SADI-S, as the small intestine remains intact, allowing for more normal nutrient absorption.
- Revisional Surgery Requirements
SADI-S may require revision in cases of severe malabsorption, unmanageable diarrhoea, or nutritional deficiencies. Conversely, SG patients may need conversion to another procedure if there is significant weight regain or if the procedure fails to provide sufficient weight loss.
- Development of worsening of acid reflux
Both SADI-S and Sleeve Gastrectomy involve the creation of a sleeve gastrectomy, where a significant portion of the stomach is removed, leaving behind a tubular-shaped stomach. This alteration in anatomy increases the risk of gastro-oesophageal reflux disease (GORD), as the higher pressure within the smaller stomach can lead to acid reflux. Because both operations share this anatomical change, they are associated with an increased risk of acid reflux, making them less suitable for patients who already have significant GORD. For individuals with pre-existing acid reflux, other bariatric procedures, such as Roux-en-Y Gastric Bypass (RYGB), may be more appropriate due to their beneficial effect on reducing acid exposure.
Both procedures emphasize the importance of lifelong follow-up and monitoring to address any complications that may arise.
Conclusion
SADI-S and Sleeve Gastrectomy each have distinct benefits and limitations. SADI-S offers greater weight loss and improved metabolic outcomes due to its stronger metabolic part. However, it comes with an increased risk of nutritional deficiencies, diarrhoea, and complications such as duodenal stump blowout.
Sleeve Gastrectomy is a simpler procedure with a lower risk of nutritional deficiencies and fewer complications related to intestinal rerouting. However, it may not provide as significant weight loss or metabolic benefits as SADI-S, particularly for patients with high BMI or uncontrolled diabetes.
Both SADI-S and Sleeve Gastrectomy narrow the stomach, creating higher internal pressure and thereby increasing the risk of acid reflux.