
Introduction
Gastric bypass surgery is a popular and effective option for individuals seeking significant weight loss and improvement in obesity-related health conditions. This article aims to provide comprehensive information about gastric bypass surgery, addressing common questions and concerns that prospective patients may have. It covers the basics of the procedure, who qualifies for it, the lifestyle changes required, and the potential risks and benefits. By offering detailed insights into what to expect before, during, and after surgery, this guide is designed to help patients make informed decisions and understand the journey towards achieving their weight loss goals.
General Information
What is gastric bypass surgery?
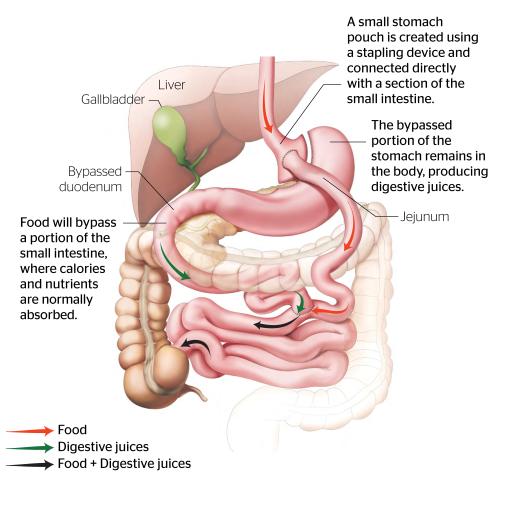
Gastric bypass surgery, particularly the Roux-en-Y type, is a bariatric procedure designed to facilitate significant weight loss by altering the digestive system. It involves creating a small stomach pouch and rerouting it to a section of the small intestine, effectively bypassing a large portion of the stomach and the initial part of the small intestine. This dual approach reduces the capacity for food intake and decreases nutrient absorption, which contributes to weight loss.
Who qualifies for gastric bypass surgery in Australia?
In Australia, gastric bypass surgery is typically indicated for individuals with a Body Mass Index (BMI) of 35 or above, or those with a BMI of 30-35 accompanied by serious obesity-related health conditions such as type 2 diabetes, hypertension, or severe sleep apnea. Suitable candidates must also demonstrate a willingness to undergo a comprehensive medical evaluation and commit to lifelong changes in diet, physical activity, and overall health management.
How much weight can I expect to lose after gastric bypass?
Weight loss outcomes vary among individuals but typically, gastric bypass patients lose about 60-80% of their excess body weight within the first two years post-surgery. Factors influencing weight loss include the type of surgery performed, initial weight, adherence to dietary recommendations, and overall lifestyle changes.
What if I want to get pregnant after gastric bypass?
It is generally recommended to wait at least 18-24 months after surgery before attempting to become pregnant. This waiting period allows your weight to stabilize and reduces the risk of nutritional deficiencies during pregnancy. Always consult with your healthcare provider to ensure a safe and healthy pregnancy plan post-surgery.
Can gastric bypass surgery cure diabetes?
Gastric bypass surgery has been shown to significantly improve, and in some cases resolve, type 2 diabetes, particularly in the immediate period following surgery. This improvement is attributed to the substantial weight loss and hormonal changes that enhance insulin sensitivity and glucose metabolism. While many patients may see a dramatic reduction or cessation of diabetes medications, continuous lifestyle management and medical monitoring are essential.
How long does the gastric bypass procedure take?
The duration of the gastric bypass procedure varies but typically lasts between one to three hours. The time required depends on the surgeon's experience, the patient's specific anatomical considerations, and whether the surgery is performed using laparoscopic or open surgical methods.
Postoperative Care and Lifestyle
What lifestyle changes are required after gastric bypass surgery?
Postoperative lifestyle changes are crucial for achieving and maintaining successful weight loss. Key adjustments include:
- Dietary Adjustments: Initially, patients begin with a liquid diet, progressing to pureed foods, and eventually to solid foods. A focus on high-protein, low-sugar, and low-fat foods is essential. Small, frequent meals are recommended to aid digestion and prevent discomfort. Ongoing supplementation of vitamins and minerals is necessary to prevent deficiencies.
- Physical Activity: Regular exercise is vital to support weight loss and maintain muscle mass. Activities should start slowly and increase gradually based on the patient’s physical capacity.
- Regular Medical Follow-ups: Routine check-ups help monitor weight loss progress, nutritional status, and any emerging complications. Consistent communication with dietitians and support groups can help maintain long-term adherence to dietary changes.
What can I eat after gastric bypass surgery?
After surgery, your diet will transition through several phases, starting with liquids only, progressing to pureed foods, and eventually to soft and then solid foods. It is crucial to concentrate on high-protein, low-sugar, and low-fat foods. Eating small, frequent meals and thoroughly chewing your food are important to facilitate digestion and prevent nutritional deficiencies. Ongoing supplementation with vitamins and minerals is typically required.
How long is the recovery period for gastric bypass surgery?
The recovery period after gastric bypass surgery varies but generally involves one to three days in the hospital followed by several weeks of home recovery. Patients typically return to normal activities within three to five weeks, depending on individual health conditions and the specifics of the surgical procedure.
Will I feel pain after surgery?
Postoperative pain is common following gastric bypass surgery, but it is typically manageable with medications prescribed by your healthcare provider. Most patients experience a significant reduction in pain within a few days after the procedure. Long-term pain is uncommon; however, any persistent discomfort should be discussed with your doctor to ensure proper management and to rule out any complications.
Are there any restrictions on my activities after surgery?
After gastric bypass surgery, patients are advised to avoid strenuous activities and heavy lifting for approximately six weeks to allow for proper healing. Gradually, patients can begin to incorporate more physical activities into their routine, following recommendations from their healthcare team. Regular exercise is an essential part of the long-term management of weight loss and overall health.
Can gastric bypass surgery affect mental health?
Gastric bypass surgery can have significant effects on mental health. While many patients experience improvements in mood and self-esteem due to weight loss and health improvements, some may struggle with adjustments to their new body image and lifestyle. Professional support from mental health experts, as well as support groups, can be beneficial in navigating these changes.
What is the typical hospital stay for gastric bypass surgery?
The typical hospital stay for gastric bypass surgery ranges from two to three days, depending on the patient's overall health, the specifics of the procedure, and the presence of any complications. Laparoscopic surgery generally allows for a shorter hospital stay and quicker recovery compared to traditional open surgery.
How does gastric bypass surgery affect medications?
Gastric bypass surgery can alter the absorption of medications due to changes in the digestive system. Some medications, particularly extended-release formulations, may need to be adjusted in dosage or switched to immediate-release forms. It's crucial to regularly review your medication regimen with your healthcare provider to ensure effective treatment and to adjust dosages as necessary to accommodate your new digestive configuration.
What are the dietary restrictions after gastric bypass surgery?
Following gastric bypass surgery, dietary restrictions typically progress from a liquid diet to pureed foods, then soft foods, and eventually regular foods over several weeks. It is essential to eat smaller portions, avoid high-sugar and high-fat foods, and thoroughly chew food. Hydration should be maintained by drinking fluids between meals, not during, to prevent stretching the new stomach size.
What are the signs of complications from gastric bypass surgery?
Potential signs of complications following gastric bypass surgery include excessive nausea and vomiting, inability to eat or drink adequately, increased abdominal pain, fever, foul-smelling drainage from any surgical incision, dark urine, light-colored stools, or jaundice. These symptoms may indicate complications such as infections, leaks, or obstructions and should prompt immediate medical attention.
What kind of follow-up care is required after gastric bypass surgery?
After gastric bypass surgery, comprehensive follow-up care is essential to ensure the patient's health and the success of the weight loss. This includes regular check-ups with the bariatric team, ongoing nutritional counseling, and monitoring for any signs of nutritional deficiencies or other health issues. Follow-up visits are typically more frequent during the first year after surgery and become annual thereafter, depending on the patient's individual needs.
How soon can I return to work after gastric bypass surgery?
Most patients are able to return to work within two to four weeks after gastric bypass surgery, depending on the nature of their job and their personal recovery. Those with physically demanding jobs may need a longer recovery period before resuming full duties.
Managing Weight and Results
How effective is gastric bypass surgery in the long term?
Gastric bypass surgery is highly effective for long-term weight loss, especially when patients follow prescribed lifestyle modifications. Most patients experience:
- 60-80% of excess body weight loss within the first two years post-surgery.
- Significant improvement in obesity-related conditions such as diabetes, hypertension, and sleep apnea.
- The long-term success of the surgery is largely dependent on the patient's commitment to maintaining dietary changes and engaging in regular physical activity.
What should I consider if I'm worried about the failure of the surgery or being disappointed with the results?
It is crucial to set realistic expectations for gastric bypass surgery. While the procedure aids in weight loss, it does not serve as a permanent solution without proper dietary and lifestyle adherence. Regular follow-up sessions with healthcare providers, including dietitians and psychologists, are vital to address and mitigate concerns about potential surgery failure or dissatisfaction with the outcomes.
How can I maintain my weight loss after gastric bypass surgery?
To maintain weight loss after gastric bypass, a lifelong commitment to healthy habits is required. Important strategies include:
- Adhering to a Nutrient-Rich Diet: Focus on a diet low in calories but rich in essential nutrients.
- Engaging in Regular Exercise: Consistent physical activity helps sustain weight loss.
- Attending Follow-up Appointments: Regular visits to healthcare providers help monitor health and adjust dietary or exercise plans.
- Seeking Support: Joining support groups or engaging with a counselor can provide motivation and address any challenges.
What happens if I start gaining weight again after surgery?
Weight regain after gastric bypass surgery can occur, particularly if dietary and exercise recommendations are not maintained. It is crucial to engage with your healthcare team if you notice weight regain. They can assist with dietary adjustments, behavioral therapy, and sometimes medication to help manage and potentially reverse the weight gain.
What should I expect in terms of weight loss progression?
Patients undergoing gastric bypass surgery generally experience rapid weight loss initially, particularly in the first six to twelve months post-operation. Following this period, weight loss tends to stabilize or plateau. The ultimate success in maintaining weight loss long-term hinges on the patient's commitment to following dietary guidelines, engaging in regular exercise, and making sustainable lifestyle adjustments.
How do I ensure the best outcomes after gastric bypass surgery?
Ensuring the best outcomes after gastric bypass surgery involves a multifaceted approach: closely following dietary and exercise recommendations provided by the healthcare team, participating in regular follow-up appointments, and engaging in support groups or psychological counseling to address any emotional or mental health challenges. Long-term commitment to these changes is crucial for maintaining weight loss and achieving overall health improvements.
What is the success rate of gastric bypass surgery?
Gastric bypass surgery is considered highly effective, with most patients maintaining substantial weight loss long-term. Studies typically show that patients lose 60-80% of their excess body weight within the first two years post-operation. Success rates are enhanced by strict adherence to dietary guidelines, lifestyle changes, and regular follow-up care to monitor health and nutritional status.
Risks and Complications
What are the potential risks and complications of gastric bypass surgery?
As with any major surgical intervention, gastric bypass surgery carries inherent risks. These include both immediate postoperative risks and potential long-term complications. Key risks include:
- Immediate Postoperative Risks:
- Infections at the surgical site.
- Bleeding.
- Adverse reactions to anesthesia.
- Long-Term Complications:
- Nutritional Deficiencies: Gastric bypass surgery alters the digestive system by bypassing parts of the stomach and small intestine, leading to decreased absorption of certain nutrients. Common deficiencies include:
- Iron: Reduced absorption due to bypassing the duodenum, the main site for iron absorption, which can lead to iron-deficiency anemia if not supplemented.
- Vitamin B12: Limited production of intrinsic factor in the smaller stomach can result in a deficiency over time, affecting energy levels.
- Calcium and Vitamin D: With reduced absorption in the duodenum and proximal jejunum, deficiencies can lead to weakened bones or osteoporosis.
- Folate and Other B Vitamins: Altered absorption in the small intestine increases the risk of deficiencies.
- Gastric Dumping Syndrome: This condition, characterized by rapid gastric emptying, can cause symptoms like diarrhea, nausea, and vomiting.
- Bowel Obstruction: A blockage in the intestines can occur, potentially requiring further surgical intervention.
- Ulcers and Hernias: These can develop at the surgical sites or along the intestinal tract.
- Nutritional Deficiencies: Gastric bypass surgery alters the digestive system by bypassing parts of the stomach and small intestine, leading to decreased absorption of certain nutrients. Common deficiencies include:
Continuous medical monitoring post-surgery is essential to manage these risks. Regular follow-up visits and adherence to a prescribed supplement regimen can help mitigate many of these complications.
Can gastric bypass surgery be reversed?
Technically, gastric bypass surgery can be reversed, but such procedures are complex and generally less common. Reversal is considered only under circumstances involving serious complications. These operations carry higher risks than the initial procedure and are not intended as solutions for patients dissatisfied with their weight loss results.
Will I need plastic surgery for the excess skin after I lose a lot of weight?
Plastic surgery to remove excess skin is commonly considered by patients who experience significant weight loss following bariatric surgery. The need for such surgery varies depending on individual factors like age, genetics, and the amount of weight lost. Typically, plastic surgery is considered after weight has stabilized, usually 18-24 months after the initial bariatric procedure.
What are the signs of complications from gastric bypass surgery?
Potential signs of complications following gastric bypass surgery include excessive nausea and vomiting, inability to eat or drink adequately, increased abdominal pain, fever, foul-smelling drainage from any surgical incision, dark urine, light-colored stools, or jaundice. These symptoms may indicate complications such as infections, leaks, or obstructions and should prompt immediate medical attention.
Gastric bypass surgery, particularly the Roux-en-Y type, is a bariatric procedure designed to facilitate significant weight loss by altering the digestive system. It involves creating a small stomach pouch and rerouting it to a section of the small intestine, effectively bypassing a large portion of the stomach and the initial part of the small intestine. This dual approach reduces the capacity for food intake and decreases nutrient absorption, which contributes to weight loss.
Who qualifies for gastric bypass surgery in Australia?
In Australia, gastric bypass surgery is typically indicated for individuals with a Body Mass Index (BMI) of 35 or above, or those with a BMI of 30-35 accompanied by serious obesity-related health conditions such as type 2 diabetes, hypertension, or severe sleep apnea. Suitable candidates must also demonstrate a willingness to undergo a comprehensive medical evaluation and commit to lifelong changes in diet, physical activity, and overall health management.
What are the potential risks and complications of gastric bypass surgery?
As with any major surgical intervention, gastric bypass surgery carries inherent risks. These include immediate postoperative risks like infections, bleeding, and adverse reactions to anesthesia. Long-term complications can include nutritional deficiencies, gastric dumping syndrome, which manifests as rapid gastric emptying causing diarrhea, nausea, and vomiting, as well as the risk of bowel obstruction, ulcers, and hernias. Continuous medical monitoring post-surgery is essential to manage these risks.
What lifestyle changes are required after gastric bypass surgery?
Postoperative lifestyle changes are critical for ensuring successful weight loss and maintenance after gastric bypass surgery. Patients are required to adhere to a structured, nutritionally balanced diet low in calories, engage in regular physical activity, and undergo routine medical follow-ups. Dietary adjustments begin with a liquid diet, progressing to pureed foods, and eventually to solid foods, with ongoing supplementation of vitamins and minerals to prevent nutritional deficiencies.
How effective is gastric bypass surgery in the long term?
Gastric bypass surgery is highly effective for long-term weight loss and significantly improves obesity-related conditions such as diabetes and hypertension. Most patients experience a loss of 60-80% of excess body weight within the first two years post-surgery. However, the long-term success of this surgery largely depends on the patient's adherence to prescribed dietary and lifestyle modifications.
What should I consider if I'm worried about the failure of the surgery or being disappointed with the results?
It is crucial to set realistic expectations for gastric bypass surgery. While the procedure aids in weight loss, it does not serve as a permanent solution without proper dietary and lifestyle adherence. Regular follow-up sessions with healthcare providers, including dietitians and psychologists, are vital to address and mitigate concerns about potential surgery failure or dissatisfaction with the outcomes.
Can gastric bypass surgery be reversed?
Technically, gastric bypass surgery can be reversed, but such procedures are complex and generally less common. Reversal is considered only under circumstances involving serious complications. These operations carry higher risks than the initial procedure and are not intended as solutions for patients dissatisfied with their weight loss results.
How much weight can I expect to lose after gastric bypass?
Weight loss outcomes vary among individuals but typically, gastric bypass patients lose about 60-80% of their excess body weight within the first two years post-surgery. Factors influencing weight loss include the type of surgery performed, initial weight, adherence to dietary recommendations, and overall lifestyle changes.
What if I want to get pregnant after bariatric surgery?
It is generally recommended to wait at least 18-24 months after surgery before attempting to become pregnant. This waiting period allows your weight to stabilize and reduces the risk of nutritional deficiencies during pregnancy. Always consult with your healthcare provider to ensure a safe and healthy pregnancy plan post-surgery.
How should I prepare for gastric bypass surgery?
Preparation for gastric bypass surgery involves several key steps: comprehensive health evaluations, lab tests, nutritional counseling, and consultations with a psychologist to prepare for the post-surgery lifestyle changes. It’s crucial to cease smoking, avoid alcohol, and adjust medications as recommended by your surgeon. Adhering to a special diet to reduce liver size and body fat is also necessary to minimize surgical risks.
What can I eat after gastric bypass surgery?
After surgery, your diet will transition through several phases, starting with liquids only, progressing to pureed foods, and eventually to soft and then solid foods. It is crucial to concentrate on high-protein, low-sugar, and low-fat foods. Eating small, frequent meals and thoroughly chewing your food are important to facilitate digestion and prevent nutritional deficiencies. Ongoing supplementation with vitamins and minerals is typically required.
How long is the recovery period for gastric bypass surgery?
The recovery period after gastric bypass surgery varies but generally involves one to three days in the hospital followed by several weeks of home recovery. Patients typically return to normal activities within three to five weeks, depending on individual health conditions and the specifics of the surgical procedure.
Will I feel pain after surgery?
Postoperative pain is common following gastric bypass surgery, but it is typically manageable with medications prescribed by your healthcare provider. Most patients experience a significant reduction in pain within a few days after the procedure. Long-term pain is uncommon; however, any persistent discomfort should be discussed with your doctor to ensure proper management and to rule out any complications.
Are there any restrictions on my activities after surgery?
After gastric bypass surgery, patients are advised to avoid strenuous activities and heavy lifting for approximately six weeks to allow for proper healing. Gradually, patients can begin to incorporate more physical activities into their routine, following recommendations from their healthcare team. Regular exercise is an essential part of the long-term management of weight loss and overall health.
Will I need plastic surgery for the excess skin after I lose a lot of weight?
Plastic surgery to remove excess skin is commonly considered by patients who experience significant weight loss following bariatric surgery. The need for such surgery varies depending on individual factors like age, genetics, and the amount of weight lost. Typically, plastic surgery is considered after weight has stabilized, usually 18-24 months after the initial bariatric procedure.
Can gastric bypass surgery cure diabetes?
Gastric bypass surgery has been shown to significantly improve, and in some cases resolve, type 2 diabetes, particularly in the immediate period following surgery. This improvement is attributed to the substantial weight loss and hormonal changes that enhance insulin sensitivity and glucose metabolism. While many patients may see a dramatic reduction or cessation of diabetes medications, continuous lifestyle management and medical monitoring are essential.
What happens if I start gaining weight again after surgery?
Weight regain after gastric bypass surgery can occur, particularly if dietary and exercise recommendations are not maintained. It is crucial to engage with your healthcare team if you notice weight regain. They can assist with dietary adjustments, behavioral therapy, and sometimes medication to help manage and potentially reverse the weight gain.
How can I maintain my weight loss after bariatric surgery?
Maintaining weight loss after bariatric surgery requires lifelong commitment to dietary management, physical activity, and overall lifestyle adjustments. It is crucial to adhere to a diet that is low in calories but rich in nutrients, engage in regular physical exercise, and attend consistent follow-up appointments with healthcare providers. Joining support groups and seeking professional help for any setbacks are also beneficial for long-term success.
Q25: What are the dietary restrictions after bariatric surgery?
Following bariatric surgery, dietary restrictions typically progress from a liquid diet to pureed foods, then soft foods, and eventually regular foods over several weeks. It is essential to eat smaller portions, avoid high-sugar and high-fat foods, and thoroughly chew food. Hydration should be maintained by drinking fluids between meals, not during, to prevent stretching the new stomach size.
How does bariatric surgery affect medications?
Bariatric surgery can alter the absorption of medications due to changes in the digestive system. Some medications, particularly extended-release formulations, may need to be adjusted in dosage or switched to immediate-release forms. It's crucial to regularly review your medication regimen with your healthcare provider to ensure effective treatment and to adjust dosages as necessary to accommodate your new digestive configuration.
What are the signs of complications from bariatric surgery?
Potential signs of complications following bariatric surgery include excessive nausea and vomiting, inability to eat or drink adequately, increased abdominal pain, fever, foul-smelling drainage from any surgical incision, dark urine, light-colored stools, or jaundice. These symptoms may indicate complications such as infections, leaks, or obstructions and should prompt immediate medical attention.
What is the success rate of gastric bypass surgery?
Gastric bypass surgery is considered highly effective, with most patients maintaining substantial weight loss long-term. Studies typically show that patients lose 60-80% of their excess body weight within the first two years post-operation. Success rates are enhanced by strict adherence to dietary guidelines, lifestyle changes, and regular follow-up care to monitor health and nutritional status.
What is the typical hospital stay for gastric bypass surgery?
The typical hospital stay for gastric bypass surgery ranges from two to three days, depending on the patient's overall health, the specifics of the procedure, and the presence of any complications. Laparoscopic surgery generally allows for a shorter hospital stay and quicker recovery compared to traditional open surgery.
What kind of follow-up care is required after gastric bypass surgery?
After gastric bypass surgery, comprehensive follow-up care is essential to ensure the patient's health and the success of the weight loss. This includes regular check-ups with the bariatric team, ongoing nutritional counseling, and monitoring for any signs of nutritional deficiencies or other health issues. Follow-up visits are typically more frequent during the first year after surgery and become annual thereafter, depending on the patient's individual needs.
How soon can I return to work after gastric bypass surgery?
Most patients are able to return to work within two to four weeks after gastric bypass surgery, depending on the nature of their job and their personal recovery. Those with physically demanding jobs may need a longer recovery period before resuming full duties.
Can gastric bypass surgery affect mental health?
Gastric bypass surgery can have significant effects on mental health. While many patients experience improvements in mood and self-esteem due to weight loss and health improvements, some may struggle with adjustments to their new body image and lifestyle. Professional support from mental health experts, as well as support groups, can be beneficial in navigating these changes.
How does gastric bypass surgery affect diabetes?
Gastric bypass surgery can have a profound impact on type 2 diabetes, often resulting in rapid improvement or remission of the disease due to significant weight loss and hormonal changes that affect insulin sensitivity and glucose metabolism. Many patients experience decreased needs for diabetes medication shortly after surgery, and some may even discontinue medications altogether under medical supervision. Continuous monitoring and adjustments by healthcare professionals are crucial to manage diabetes effectively post-surgery
How long does the gastric bypass procedure take?
The duration of the gastric bypass procedure varies but typically lasts between one to three hours. The time required depends on the surgeon's experience, the patient's specific anatomical considerations, and whether the surgery is performed using laparoscopic or open surgical methods.
What should I expect in terms of weight loss progression?
Patients undergoing gastric bypass surgery generally experience rapid weight loss initially, particularly in the first six to twelve months post-operation. Following this period, weight loss tends to stabilize or plateau. The ultimate success in maintaining weight loss long-term hinges on the patient's commitment to following dietary guidelines, engaging in regular exercise, and making sustainable lifestyle adjustments.
How do I ensure the best outcomes after gastric bypass surgery?
Ensuring the best outcomes after gastric bypass surgery involves a multifaceted approach: closely following dietary and exercise recommendations provided by the healthcare team, participating in regular follow-up appointments, and engaging in support groups or psychological counseling to address any emotional or mental health challenges. Long-term commitment to these changes is crucial for maintaining weight loss and achieving overall health improvements.
 The Roux-en-Y Gastric Bypass works through a combined mechanism of restriction and significant metabolic changes. By creating a small pouch from the upper part of the stomach, the surgery naturally limits the amount of food that can be consumed at any one time, enforcing a physical restriction on calorie intake. Simultaneously, the procedure induces profound metabolic changes by rerouting the food pathway directly to a section of the small intestine. This alteration triggers hormonal changes that enhance feelings of satiety, decrease hunger, and significantly improve metabolic disorders such as type 2 diabetes.
The Roux-en-Y Gastric Bypass works through a combined mechanism of restriction and significant metabolic changes. By creating a small pouch from the upper part of the stomach, the surgery naturally limits the amount of food that can be consumed at any one time, enforcing a physical restriction on calorie intake. Simultaneously, the procedure induces profound metabolic changes by rerouting the food pathway directly to a section of the small intestine. This alteration triggers hormonal changes that enhance feelings of satiety, decrease hunger, and significantly improve metabolic disorders such as type 2 diabetes.
Old vs New Concepts
The RYGB is often desctribed as restrictive and malabsorptive operation. It is important to understand that this is not true. Though there is degree of fat malabsortion in RYGB, the amount of fat not absorbed is trivial. The RYGB works by making us eat less via some restriction and significant metabolic effects.
The Metabolic Effects of Roux en Y Gastric Bypass
The metabolic effects of Roux-en-Y Gastric Bypass (RYGB) operation are profound and contribute significantly to its effectiveness in promoting weight loss and improving metabolic disorders, such as type 2 diabetes. Two prominent theories, the Foregut Hypothesis and the Hindgut Hypothesis, have been proposed to explain these effects, shedding light on the complex interactions between the gastrointestinal tract and metabolic regulation.
Foregut Hypothesis
The Foregut Hypothesis suggests that the RYGB operation leads to weight loss and metabolic improvements by bypassing the upper part of the small intestine, known as the foregut. According to this theory, the foregut produces signals that negatively affect insulin sensitivity and glucose metabolism when food is ingested. By rerouting food directly from the stomach to the mid-section of the small intestine, RYGB operation might reduce the secretion or the effect of these diabetogenic signals thereby enhancing insulin sensitivity and promoting a more favorable metabolic profile. This hypothesis underscores the importance of what is being bypassed in the procedure, suggesting that the exclusion of the foregut from the digestive process plays a critical role in the metabolic benefits observed after RYGB.
Hindgut Hypothesis
Conversely, the Hindgut Hypothesis focuses on the accelerated delivery of nutrients to the lower part of the small intestine, known as the hindgut, following RYGB operaton. This rapid nutrient delivery is thought to stimulate the increased secretion of anti-diabetogenic signals, such as glucagon-like peptide-1 (GLP-1) and peptide YY (PYY), hormones that are known to enhance insulin secretion, inhibit glucagon release, slow gastric emptying, and reduce appetite. The enhanced anti-diabetogenic effect is believed to contribute significantly to the improvements in glucose homeostasis and the reduction of appetite, leading to weight loss. This hypothesis highlights the beneficial effects of stimulating the hindgut and the role of incretins in mediating the metabolic improvements post-RYGB.
Both the Foregut and Hindgut Hypotheses offer valuable insights into the complex mechanisms through which RYGB surgery exerts its metabolic effects. These theories are not mutually exclusive and may both contribute to the profound changes observed in patients undergoing this procedure.
Effect of Roux en Y Gastric Bypass on Bile Salts
Bile salts, which are critical for the digestion and absorption of fats, have also been recognized for their role in metabolic regulation, particularly after bariatric surgery.
Following RYGB, there is a notable alteration in the bile acid pool size and composition, as well as changes in the flow of bile acids through the gastrointestinal tract. These changes have profound metabolic implications, contributing to the surgery's effectiveness in weight loss and blood glucose control.
- Enhanced GLP-1 Secretion: The altered flow of bile acids to the distal intestine post-RYGB increases the secretion of glucagon-like peptide 1 (GLP-1), a hormone that plays a vital role in insulin secretion, glucose homeostasis, and satiety.
- Altered Gut Microbiota: Bile acids influence the composition of the gut microbiota. Changes in bile acid circulation after RYGB can lead to shifts in the gut bacterial populations, which in turn affect metabolic health.
- Activation of Bile Acid Receptors: Bile acids act as signaling molecules through specific receptors, such as the farnesoid X receptor (FXR) and the G protein-coupled bile acid receptor (TGR5). Activation of these receptors plays a crucial role in glucose, lipid, and energy metabolism.
- Energy Expenditure: There is evidence to suggest that changes in bile acid circulation post-RYGB can lead to increased energy expenditure.
Effects of Roux en Y Gastric Bypass on Gut Bacteria
The gut microbiota, comprising trillions of microorganisms, including bacteria, viruses, and fungi, plays a crucial role in digesting food, regulating the immune system, and protecting against pathogens. Importantly, these microscopic inhabitants also exert profound effects on body weight and fat storage.
After RYGB, patients typically experience substantial changes in the diversity and abundance of their gut microbiota. These changes are characterized by:
- Increased Diversity: There is often an increase in the overall diversity of the gut microbiota, which is generally considered beneficial for health. Higher bacterial diversity is associated with improved metabolic health and reduced risk of obesity and certain chronic diseases.
- Shifts in Bacterial Populations: Specific shifts in bacterial populations occur, including an increase in certain beneficial bacteria known for their positive metabolic effects, such as those producing short-chain fatty acids (SCFAs). SCFAs, including butyrate, propionate, and acetate, play crucial roles in maintaining gut health, regulating inflammation, and influencing energy metabolism.
- Reduction in Harmful Bacteria: Reductions in the abundance of bacteria associated with inflammation and metabolic dysregulation have also been observed. These changes can contribute to the overall anti-inflammatory and metabolic benefits of RYGB.
 The Roux-en-Y Gastric Bypass (RYGB) is unique among all other bariatric operations for its ability to improve Gastro-Oesophageal Reflux Disease (GORD) while also promoting weight loss. In contrast, other bariatric operations can potentially worsen GORD. This improvement is achieved through multiple mechanisms, directly resulting from the surgical alterations made during the procedure.
The Roux-en-Y Gastric Bypass (RYGB) is unique among all other bariatric operations for its ability to improve Gastro-Oesophageal Reflux Disease (GORD) while also promoting weight loss. In contrast, other bariatric operations can potentially worsen GORD. This improvement is achieved through multiple mechanisms, directly resulting from the surgical alterations made during the procedure.
Mechanisms of GORD Improvement in RYGB
- Weight Loss:
One of the primary mechanisms by which RYGB helps alleviate GORD is through significant weight loss. The reduction of body weight decreases intra-abdominal pressure, a major contributing factor to GORD. Lower abdominal pressure reduces the likelihood of stomach contents being pushed back up into the oesophagus, thereby lessening reflux symptoms. - Anatomical Changes:
RYGB surgery fundamentally changes the anatomy of the stomach, creating a smaller stomach pouch that holds less food and produces less gastric acid. The reduction in stomach size and acid production significantly decreases the volume and potency of refluxed material, thereby minimising damage to the oesophageal lining. - Reduction in Stomach Pouch Pressure:
By surgically connecting the small stomach pouch directly to the intestine, RYGB reduces the pressure within the pouch. This anatomical alteration prevents the buildup of excessive pressure that could otherwise force stomach contents upward into the oesophagus, further reducing the risk of acid reflux. - Prevention of Bile Reflux:
The configuration of the RYGB includes a critical second anastomosis approximately 60-100cm downstream from where the stomach pouch connects to the intestine. This design ensures that bile, which can be highly irritating to the oesophageal lining, does not reach the stomach pouch or oesophagus. By preventing bile reflux, RYGB offers a distinct advantage over other types of bariatric surgery, such as the One Anastomosis Gastric Bypass (OAGB), in managing GORD.
The Roux-en-Y Gastric Bypass not only facilitates significant weight loss but also incorporates specific anatomical changes that collectively improve symptoms of Gastro-Oesophageal Reflux Disease. The surgery reduces both the causes and the effects of acid reflux, making it a favourable option for patients with severe GORD alongside obesity.
The Roux-en-Y Gastric Bypass (RYGB) is a bariatric operation designed to facilitate substantial weight loss by modifying the stomach and the small intesine. In this procedure, a small pouch is created from the upper section of the stomach, significantly limiting food intake. This newly formed pouch is then connected directly to a section of the small intestine, essentially bypassing the majority of the stomach and a significant portion of the small intestine. This rerouting is achieved through two critical connections or "anastomoses": one where the small stomach pouch is joined to the small intestine, and another further down where the bypassed portion of the stomach and upper intestine is reattached to the small intestine.
Absorption Before and After Roux en-Y Gastric Bypass Surgery
Normal Absorption Before Gastric Bypass
Stomach: The stomach primarily initiates the digestion of proteins through the action of gastric acid and enzymes like pepsin. The stomach acid convert iron and calcium to forms that is easier for the intestine to absorb. The stomach also secrets the interinsic factor. This binds Vitmain B12 facilitating its absorption by the small intestine. The stomach does not absrob much.
Proximal Small Intestine (Duodenum and Jejunum): This is where a significant portion of nutrient absorption occurs. The duodenum and jejunum are primarily responsible for the absorption of iron, calcium, magnesium, and the majority of vitamins, including fat-soluble vitamins (A, D, E, K). The proximal small intestine also absorbs most carbohydrates, proteins, and lipids.
Rest of the Intestine (Ileum and Large Intestine): The ileum continues the absorption of nutrients not absorbed by the jejunum, including vitamin B12 and bile acids, which are critical for fat digestion. The ileum and large intestine also absorb water and electrolytes.
Changes in Absorption After Roux en-Y Gastric Bypass Surgery
Macronutrient Absorption:
Proteins: The altered pH and reduced stomach size after RYGB can impact protein digestion, as less gastric acid and pepsin are available. This might lead to slightly reduced efficiency in protein absorption, particularly in the early postoperative period. However, most patients can absorb enough protein from the adapted small intestine with proper dietary intake.
Carbohyrdate: absorption of carbohydrates is usually not affected.
Fats: Fat absorption is more significantly impacted due to bypassing the duodenum and jejunum, where most fat digestion and absorption occur. The reduced emulsification by bile acids (due to altered bile flow) and decreased lipase activity can lead to steatorrhea (fat in the stool) and contribute to fat-soluble vitamin deficiencies.
Micronutrient Absorption:
Iron and Calcium: These minerals are primarily absorbed in the duodenum, which is bypassed in RYGB. Reduced stomach acid also decreases iron's conversion to its more absorbable form, leading to an increased risk of anemia. Calcium absorption is similarly affected, increasing the risk of osteoporosis.
Vitamins: The absorption of fat-soluble vitamins (A, D, E, K) is compromised due to decreased fat absorption. Vitamin B12 absorption is also impacted due to bypassing parts of the stomach that produce intrinsic factor, essential for its absorption in the ileum.
Other Micronutrients: The absorption of other micronutrients like magnesium and zinc can also be affected, given their absorption sites are in the regions of the intestine that are bypassed or altered.
Patients require lifelong supplementation of vitamins and minerals, particularly those whose absorption has been most affected, to prevent deficiencies and associated complications.
Advantages of Roux en-Y Gastric Bypass
- Significant and Sustained Weight Loss: RYGB typically results in substantial long-term weight loss, helping patients lose up to 70% of their excess weight. This dramatic reduction can significantly decrease the risk of mortality associated with obesity.
- Resolution of Comorbidities: The procedure has a profound impact on obesity-related health conditions. Diabetes remission rates are notably high, with many patients experiencing improved or normalized blood sugar levels. Hypertension, obstructive sleep apnea, and dyslipidemia also improve or resolve in a majority of patients.
- Metabolic Benefits: The surgery induces significant metabolic improvements, including changes in gut hormones that lead to reduced appetite and increased satiety, making it easier for patients to adhere to healthier dietary patterns.
- Improvement in acid reflux or GORD: One of the notable advantages of Roux-en-Y Gastric Bypass (RYGB) operaton over all other bariatric operations is its beneficial effect on Gastroesophageal Reflux Disease (acid reflux). This is achieved by several mechanisms.
- Weight Loss: The substantial weight loss that follows RYGB reduces intra-abdominal pressure, one of the key contributors to GORD.
- Anatomical Changes: RYGB alters the stomach's anatomy, significantly reducing the stomach size and, consequently, the amount of acid produced. Anatomical Changes: RYGB alters the stomach's anatomy, significantly reducing the stomach size and, consequently, the amount of acid produced.
- Reduction in pressure inside the stomach pouch: By joining the small stomach pouch to the intestine this reduces the pressure inside the stomach pouch thus less pressure to drive acid the wrong way up into the oesophaugs.
- No bile reflux: the second joint in RYGB is done about 60-100cm down stream from the stomach pouch joint. This ensures that no bile reaches the stomach pouch and thus oesopahgus. This is one of the main advantages of RYGB over OAGB.
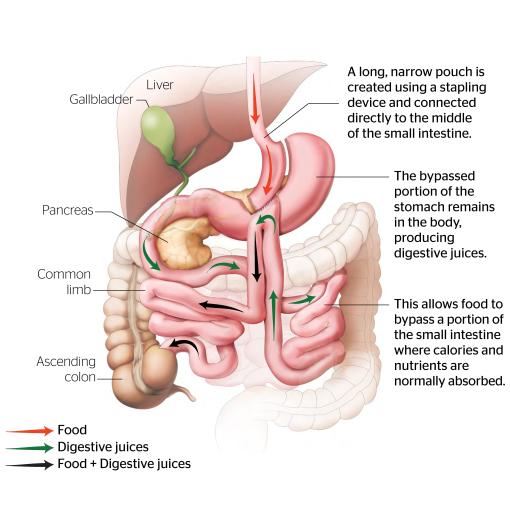
This minimally invasive procedure involves creating a long, narrow tube from the stomach and connecting it directly to a loop of the small intestine, bypassing a large portion of the stomach and the first part of the small intestine. This design reduces the amount of food the stomach can hold and decreases the absorption of calories and nutrients, leading to weight loss.
This operation was first described in 2001 and it is currently the third most frequently performed bariatric worldwide after sleeve gastectomy and roux en y gastric bypass. It will likely over take roux en y gastric bypass in the future.
The one anastmosis gastric bypass OAGB is also referred to as mini gastric bypass or omega loop gastric bypass or single anastomsis gastric bypass. It is important to understand that the name mini gastric bypass is not because it is minor operation but rather because, when it was original described, part of the operation was done via a small or "mini" laparotomy (open mindline cut).
How does OAGB work?
OAGB induces weight loss through two primary mechanisms: restriction and metabolic changes. The surgical creation of a smaller stomach pouch limits the volume of food that can be consumed at one sitting, fostering an early sense of satiety. More profoundly, the procedure modifies the normal digestive process by allowing unaltered food to enter the intestine further along than it normally would. This triggers hormonal and receptor changes within the body, enhancing satiety, and optimizing energy utilization. In addition there is a small degree of fat malabsorption.
Benefits of OAGB
The benefits of OAGB extend beyond substantial weight loss. Patients often experience improvements in obesity-related conditions such as type 2 diabetes, hypertension, sleep apnea, and high cholesterol.
Typical Weight Loss Outcomes
Patients undergoing OAGB can expect to lose between 60% to 80% of their excess body weight within the first two years post-surgery. It's important to note that individual results may vary, and maintaining weight loss will require adherence to a healthy diet and regular physical activity.
Advantages of OAGB Over Sleeve Gastrectomy
Greater Weight Loss Potential: OAGB often results in a higher percentage of excess weight loss compared to Sleeve Gastrectomy, primarily due to its stronger metabolic effect than in sleeve gastrectomy.
Improvement in Metabolic Conditions: Patients undergoing OAGB may see a more significant improvement in obesity-related conditions such as type 2 diabetes, hypertension, and hyperlipidemia, attributed to the metabolic changes induced by the procedure.
Reversibility: Unlike the Sleeve Gastrectomy, which permanently removes a portion of the stomach, the OAGB is potentially reversible, offering more flexibility in managing long-term outcomes and complications.
Disadvantages of OAGB Over Sleeve Gastrectomy
Nutritional Deficiencies: OAGB carries a higher risk of nutritional deficiencies due to the malabsorption caused by bypassing a portion of the small intestine. This requires patients to commit to lifelong nutritional supplementation and monitoring.
Risk of Bile Reflux: There is a concern about the risk of bile reflux gastritis in OAGB patients, a condition where bile flows into the stomach, causing discomfort and potential damage to the stomach lining. This risk is less prevalent in Sleeve Gastrectomy since the pylorus is kept intact, regulating the entry of bile into the intestine.
Complexity of the Procedure: Although OAGB is considered less complex than traditional Roux-en-Y gastric bypass, it is still more complex than the Sleeve Gastrectomy.
Risk of Marginal Ulcer and Bowel Twist: Unique to gastric bypss, there is a risk of developing marginal ulcers at the site where the small intestine is connected to the stomach. Additionally, OAGB patients may experience a higher risk of bowel twist (intestinal obstruction) compared to those who undergo Sleeve Gastrectomy, which does not involve any alteration to the small intestine's routing.
Possible Dumping Syndrome: Gastric bypass patients might experience dumping syndrome, a condition characterized by rapid gastric emptying leading to symptoms like nausea, vomiting, diarrhea, dizziness, and sweating. This syndrome is more common in procedures that alter the normal flow of food through the gastrointestinal tract, including OAGB, but is less likely with Sleeve Gastrectomy.
Limitations on Endoscopic Procedures: After undergoing OAGB, as well as Roux-en-Y Gastric Bypass (RYGB),ERCP become nearly impossible due to the altered gastrointestinal anatomy. ERCP is a specialized endoscopy used to diagnose and treat conditions in the liver, gallbladder, bile ducts, and pancreas. The procedure involves the insertion of an endoscope through the mouth, down the stomach, and into the first part small intestine to reach the biliary and pancreatic ducts. After OAGB and RYGB, the bypassed proximal small bowel and the reconfiguration of the gastrointestinal tract prevent the standard approach to ERCP, complicating the management of biliary and pancreatic diseases.
Advantages of OAGB Over Roux-en-Y Gastric Bypass
Simpler Surgical Procedure: OAGB involves a less complex surgical technique with only one anastomosis (connection) between the stomach and the small intestine. This simplicity can lead to shorter operating times and potentially lower risks of surgical complications compared to the RYGB, which involves creating two anastomoses.
Faster Recovery and Shorter Hospital Stay: Due to its less invasive nature, patients undergoing OAGB often experience faster recovery times and may have shorter hospital stays compared to those who undergo RYGB.
Comparable or Superior Weight Loss Outcomes: Several studies have shown that OAGB can achieve comparable, if not superior, weight loss outcomes in the long term compared to RYGB.
Improvements in Metabolic Syndrome: OAGB has been effective in improving, and in some cases resolving, metabolic syndrome and its components, such as type 2 diabetes, hypertension, and hyperlipidemia. The metabolic benefits of OAGB can be attributed to the hormonal changes induced by the surgery, which are similar to or even greater than those seen with RYGB.
Potential for Reversal and Adjustability: Unlike RYGB, which is more challenging to reverse, OAGB offers the potential for reversibility and adjustability. This can be an essential advantage for patients who may require modifications to their initial surgery due to nutritional deficiencies or inadequate weight loss.
Lower Risk of Internal Hernias and bowel twist: The design of the OAGB procedure creates only one mesenteric defect, as opposed to the RYGB, which creates two mesenteric spaces due to its more complex intestinal rerouting. Internal hernias occur when intestines protrude through these mesenteric defects, a situation that can lead to serious complications requiring emergency surgery. The simpler configuration of OAGB minimizes the likelihood of such protrusions by limiting the potential spaces through which the intestines could herniate.
Disadvantages of OAGB Compared to RYGB
Risk of Bile Reflux: One of the primary concerns with OAGB is the increased risk of bile reflux gastritis. In OAGB, the rerouting of the digestive tract can allow bile to flow back into the stomach and esophagus, leading to inflammation, discomfort, and potential damage to the gastric and esophageal lining. This does not occur after RNYGB due to presence of the second joint.
Malnutrition and Nutritional Deficiencies: Although both operations alter nutrient absorption, the risk of malnutrition and nutritional deficiencies can be higher in OAGB patients. This is due to the more extensive bypass of the small intestine in OAGB, which affects the absorption of vitamins, minerals, and nutrients more significantly than RYGB.
Risk of Marginal Ulceration: Patients who undergo OAGB have an increased risk of developing marginal ulcers at the site where the stomach is connected to the small intestine. Although this is a risk with RYGB as well, the potential for ulcer formation may be higher in OAGB due to the large gastric pouch in OAGB producing more acid than the smaller pouch of RNYGB.
Variations in OAGB: The Length of the Biliopancreatic Limb
In performing OAGB, surgeons may opt for a "conservative" 150cm BP limb or a "standard" 200cm BP limb. Some centers might even extend the BP limb length to 250cm or more, based on their clinical judgment and the specific needs of the patient. This variation reflects the lack of consensus within the bariatric surgrey community regarding the optimal BP limb length for maximizing weight loss while minimizing complications. The choice of limb length often depends on factors such as the patient's Body Mass Index (BMI) or the total length of the alimentary limb, with some surgeons preferring longer lengths for individuals with a BMI over 50.
There is evidence that 150 cm BP limb might be the best choice for the following reasions:
Safe and effective in the medium term: This length has shown good results in terms of weight loss and improvement in comorbidities.
Not associated with a poorer weight loss outcome compared to the 200cm OAGB, even in patients with a BMI greater than 50.
Potentially lower risk of protein-calorie malnutrition and micronutrient/vitamin deficiencies: Longer BP limbs may increase the risk of these nutritional issues due to the greater extent of malabsorption.